
The American health care system is beset with inequalities that have a disproportionate impact on people of color and other marginalized groups. These inequalities contribute to gaps in health insurance coverage, uneven access to services, and poorer health outcomes among certain populations. African Americans bear the brunt of these health care challenges.
African Americans comprise 13.4 percent of the U.S. population.1 Over the span of several decades, namely since the Civil Rights Acts of 1964 and 1968, they have been able to make notable strides in American society. According to the Economic Policy Institute, educational attainment has greatly increased, with more than 90 percent of African Americans aged 25–29 having graduated from high school.2 College graduation rates have also improved among African Americans. When it comes to income, gains have been made as well, but African Americans are still paid less than white Americans for the same jobs and lag significantly behind when it comes to accumulating wealth. And as for home ownership, just over 40 percent of African Americans own a home—a rate virtually unchanged since 1968.3
African Americans are also living longer, and the majority of them have some form of health insurance coverage. However, African Americans still experience illness and infirmity at extremely high rates and have lower life expectancy than other racial and ethnic groups. They are also one of the most economically disadvantaged demographics in this country.
This report will examine the state of health care coverage for African Americans and shed a light on important social factors that uniquely impact their health outcomes. In an effort to draw implications from leading health care reform plans, recommendations are made for the way forward in ensuring that the physiological and social impacts of racism are not omitted in efforts to secure truly universal health care coverage in America. African Americans are one of the most politically engaged demographics in this country. Addressing their unique challenges and perspectives, including the pervasive impacts of racism, must be included in health reform efforts.
Coverage Gains—and Obstacles—for African Americans Under the ACA
The Affordable Care Act (ACA) has helped to ensure health care coverage for millions of Americans. The uninsured rate among African Americans declined after the law was implemented: of the more than 20 million people who have gained coverage under the ACA, 2.8 million of them are African-American.4 Yet, this population is still more likely to be uninsured than white Americans: as of 2018, the uninsured rate among African Americans was 9.7 percent, while it was just 5.4 percent among whites.5 African Americans were more likely to be covered through employer-sponsored or private health insurance: 55 percent of African Americans used private health insurance in 2018, while 41.2 percent were enrolled in Medicaid or some other type of public health insurance.6
While coverage expansions under the ACA have hastened the progress toward universal coverage, the continued high cost of many coverage options means that access to affordable health care is still a challenge for many Americans—particularly African Americans.
The average family spends $8,200 (or 11 percent of family income) per year on health care premiums, and out-of-pocket costs for things such as office visit copays, prescription drugs, and surprise or out of plan medical bills continue to wreak havoc on the financial security of families.7 For African Americans, the average annual cost for health care premiums is almost 20 percent8 of the average household income—a major cost to bear, when taking into account income inequality and other economic challenges for this demographic.
The high cost of coverage has kept the number of uninsured and underinsured unacceptably high: of the 27.5 million people that still lack health insurance coverage,9 45 percent cite cost as the reason for being uninsured.10 Furthermore, the Commonwealth Fund estimates that an additional 87 million people (adults aged 19 to 64) are underinsured; that is, they have coverage, but their plan leads to unusually high out-of-pocket costs relative to income that can lead to a strain on personal finances or even debt. Of these underinsured adults, 18 percent are African-American.11
Systemic Health Care Challenges That Reform Must Address
Despite coverage gains, remaining health care challenges exist that have a disproportionate impact on African Americans. The lack of Medicaid expansion in key states, health disparities, and health care provider shortages make it incredibly hard to address America’s health care needs in a comprehensive way. And while these challenges are factors that touch many Americans in various parts of the country, the gravity of them is uniquely seen in the South, and among the African-American population.
The South’s Stubborn Approach to Medicaid Expansion
The Medicaid program has been a lifeline for low-income Americans, pregnant people, the elderly, and people with disabilities. It is jointly funded by states and the federal government, and has been operating for fifty-four years.12 As of August 2019, the program covered 68 million people, with African Americans making up about 20 percent of Medicaid enrollees.13 Because African Americans tend to be poorer than other demographic groups on average, public health insurance programs such as Medicaid are vital to ensure affordable health care and healthier outcomes. In states that have not expanded Medicaid under the Affordable Care Act (ACA), African Americans and other people of color are most likely to fall within a coverage gap—meaning they earn too much to qualify for the traditional Medicaid program, yet not enough to be eligible for premium tax credits under marketplace plans.14
The states that have not expanded Medicaid are largely concentrated in the southern region of the United States.
Under the ACA, Medicaid eligibility was expanded for adults with incomes up to 138 percent of the federal poverty level (FPL).15 This expansion was originally written into the ACA as a requirement for all states, but due to a 2012 Supreme Court ruling in National Federation of Independent Business v. Sebelius,16 it is now just an option for states. To date, thirty-seven states (including the District of Columbia) have expanded Medicaid, either through traditional means or the Section 1115 waiver process.17 The states that have not expanded Medicaid are largely concentrated in the southern region of the United States. (See Map 1.)
Map 1
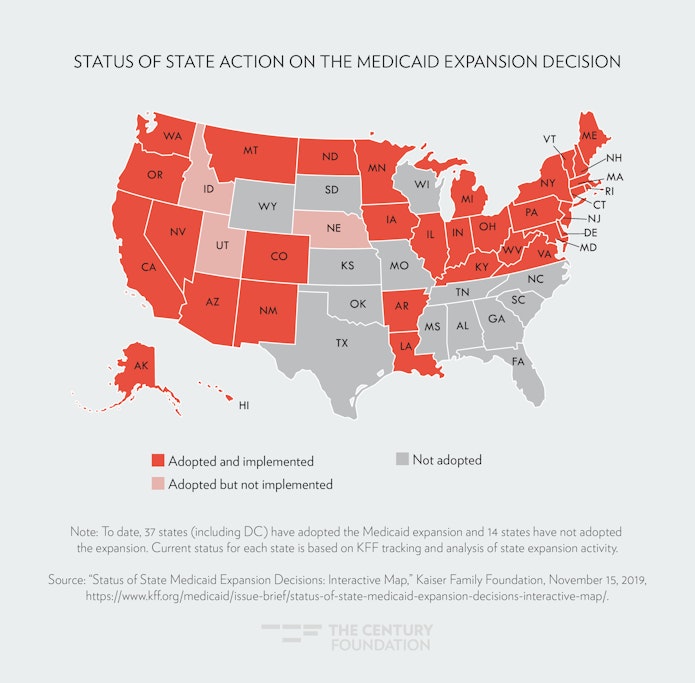
In the South, African Americans are disproportionately represented. According to the U.S. Department of Health and Human Services Office of Minority Health, 58 percent of the African-American population lived in the South as of 2017.18 They are also more likely to be uninsured, with Texas, Florida, and Georgia being home to the largest shares of uninsured African Americans.19 Some states have also proposed draconian work requirements20 as a condition for the participation in the Medicaid program. These requirements can only serve to stigmatize enrollees, deny coverage, and discourage low-income people from the support they desperately need. In Arkansas—one of nine states to date with 1115 waivers approved by the Trump administration allowing fully implemented work requirements—18,000 low-income people lost health care coverage as a result.21 This coverage loss comes as no surprise, because the use of work requirements for other safety-net programs, including Temporary Assistance for Needy Families (TANF), has proven them to be ineffective in their stated goal—promoting employment—yet highly effective in reducing program eligibility.22 Medicaid work requirements for three states have been struck down by the courts. Due to the failure to expand Medicaid, the South is now home to the nation’s sickest people, and is where health disparities between whites and people of color are the most pronounced.23
Disparities in Health Outcomes
Increases in health insurance coverage under the ACA have improved access to medical care and have been linked to better outcomes for African Americans, such as earlier diagnosis and treatment of certain cancers.24 However, disparities still exist across health conditions when comparing African Americans and whites, including maternal mortality, infant mortality, heart disease, diabetes, cancer, and other health issues. Social factors, including economic disadvantage, inequities in education, and lack of access to health care, impact a person’s ability to lead a healthy and productive life. For people in American society that experience racism and inequality in their daily lives, and throughout the lifespan, the impact of social factors on health are the most grave.
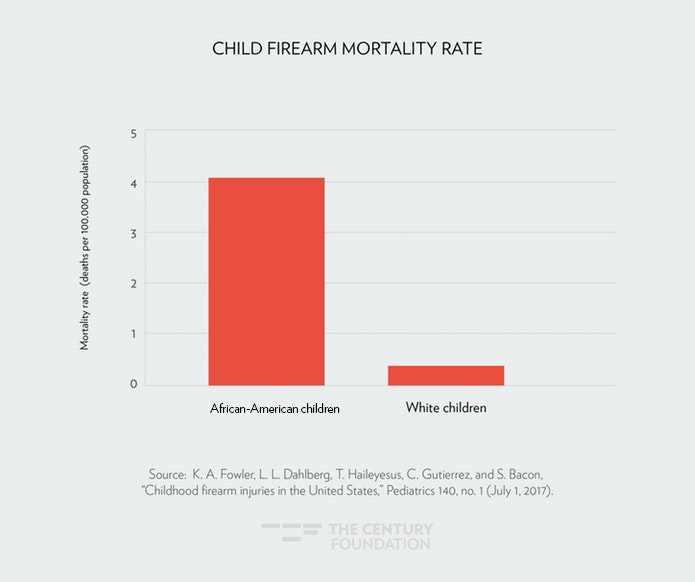
Even with improved access to medical care under the ACA, the disparities in health outcomes between African Americans and whites are stark. African-American women are three times more likely to die of pregnancy-related causes than white women (see Figure 1).25 The African-American infant mortality rate is twice the rate for white infants (see Figure 2).26 African Americans are more likely to die from cancer and heart disease than whites, and are at greater risk for the onset of diabetes.27 However, death rates for African Americans with cancer and heart disease did drop over a fifteen year period.28 Across many chronic illnesses, however, African Americans are still more likely to die compared to other racial and ethnic groups. Homicides are also a leading cause of death for African Americans. In fact, African American children are ten times more likely to die by gun violence than white children (see Figure 3).29
Figure 1
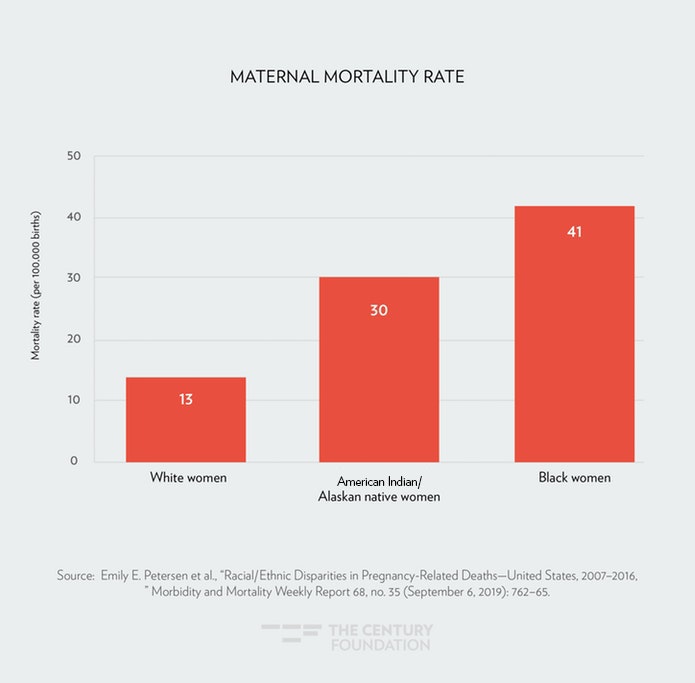
Figure 2
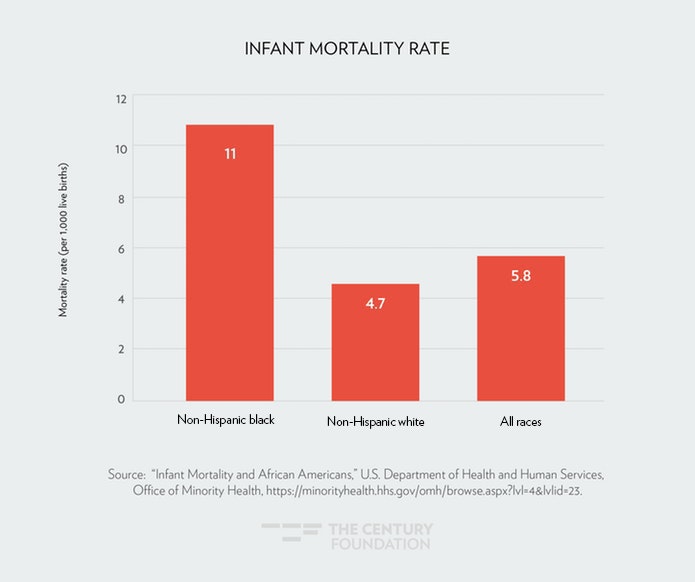
Figure 3
Health Care Provider Shortages
Due to residential segregation, majority African-American and Hispanic areas are more likely to lack hospitals and other health care providers.30 Therefore, place matters. When health care providers are located within majority African-American and Hispanic neighborhoods, they tend to offer lower-quality care.31 Often, people of color find themselves relying heavily on community health centers, emergency rooms or outpatient care, and community-based providers due to the lack of available primary care and mental health providers in a given geographic area. Traveling outside of the immediate geographic area to access health care may be an option for some people, yet this can be a challenge due to lack of access to transportation for those with limited incomes or for those living in rural areas.
It is not difficult to locate where—and for whom—provider shortages are a serious concern. The Health Resources and Services Administration (HRSA) defines Health Professional Shortage Areas (HPSAs) as geographic, population, or facility-based designations that are indicative of health care provider shortages.32 Designations are made by the following health disciplines: primary care, dental health, and mental health. Federal regulations dictate the threshold for shortages by calculating the ratio of population to provider in order to identify high need areas.33 In 2018, there were 17,657 geographic areas, populations, and facilities identified by HRSA as not having enough health care providers.34 Mental health and primary care were the disciplines in the shortest supply.
Medically Underserved Areas and Populations (MUA/Ps) are another designation by HRSA. They are geographic areas and populations that lack adequate access to primary care providers.35 MUA/Ps identify specific populations that are likely to experience barriers to health care including the homeless, low-income people, people eligible for Medicaid, Native Americans, and migrant farmworkers. Designations are made by calculating the population-to-provider ratio, percent of population below the federal poverty level, percent of population over the age of 65, and the infant mortality rate.36
Important Considerations for Health Care Specific to African Americans
Certain social factors, also referred to as social determinants of health, have important implications for health risk and the ability to attain health insurance coverage. Poverty, income inequality, wealth inequality, food insecurity, and the lack of safe, affordable housing are just a few. Another important social factor leading to poor health outcomes and economic disadvantage among African Americans is racism, because not only is it a stressor, but it impacts who gets what in America, particularly health care.
Racism’s Wear and Tear on African Americans
African Americans have endured racism within American society for hundreds of years. Studies conducted over time have been consistent in proving that racism not only impacts social stratification, but also the ability of African Americans to be healthy—both mentally and physically.37 This burden—a burden that is indeed inescapable for black and brown people in this country—causes African Americans to die prematurely and experience chronic illnesses and mental health challenges at higher rates than white Americans.
According to a study published in the journal of Psychoneuroendocrinology, racist experiences bring on an increase in inflammation in African Americans.38 This increase in inflammation raises the risk of becoming chronically ill. The researchers of the study assert that, because the body’s response to stressors—such as the adversity of racism—results in compromising systems that are critical in fending off disease, exposure to racism over long periods of time caused the health of African Americans to suffer greatly with chronic illness as the body’s defenses were down due to inflammation.39 Chronic illnesses associated with experiencing racism include heart attack, neurodegenerative disease, and metastatic cancer.40 The study participants had similar socioeconomic backgrounds, which eliminated poverty as a stressor—a social factor that has also been linked to the onset of illness.
Similar findings were yielded in some of the earliest studies looking at the impact of racism on the health of African Americans by University of Michigan public health researcher Arline Geronimous. After looking at biological factors associated with exposure to stressors, Geronimous hypothesized, in what is also referred to as the weathering hypothesis, that African Americans experienced health deterioration because of those stressors.41 Geronimous examined the allostatic load scores—that is, the cumulative wear and tear on the body’s system brought on by the repeated adaptation to stressors42—for adults aged 18–64. African Americans were found to have higher scores than white Americans. Once again, poverty was ruled out as a factor, due to the fact that the higher allostatic loads existed among African Americans of various socioeconomic backgrounds. Geronimous concluded that racism, and the burden of coping with it across the lifespan, leads to differences in health among African Americans and white Americans—including the onset of chronic illness and premature death.
In addition to instigating poor health outcomes among African Americans, racism also creates barriers to economic opportunity and uneven access to health care. Even the health care system itself perpetuates racism and bias43 toward African Americans. This has been well documented with examples, including differences in pain management and treatment of African Americans when compared to whites experiencing the same health conditions, use of African Americans’ bodies in medical experimentation, and racial bias in health algorithms for the purpose of guiding health decisions and assessing health care costs.44 Actions like these have led to a general distrust of the health care system within the African American community.45 Racism cannot be divorced from the other social factors outlined in this report, which give reason to the fact that African Americans are disproportionately affected by them.
Poverty
Across economic indicators, vast disparities exist between African Americans and whites that mirror the proportions seen in health disparities. Due to structural barriers, African Americans are more likely to be poor than white Americans and are less likely to have a full-time worker in the household.46 The poverty rate among African Americans was 20.8 percent in 2018, higher than for any other racial or ethnic group in the United States, and more than twice the poverty rate of white Americans.47 Growing up in poverty is also associated with toxic stress,48 of which the impact can reach crisis levels when a person is also grappling with the toxic stress brought on by racism. When African Americans are able to attain work, they are more likely to work in low-paying jobs that lack important benefits, including health insurance and paid leave. The African-American poverty rate also shows how critical public programs such as Medicaid are to helping ensure access to health care for this population. Because of these factors, Medicaid expansion helps more African Americans gain coverage than any other group.49
Household Income Inequality
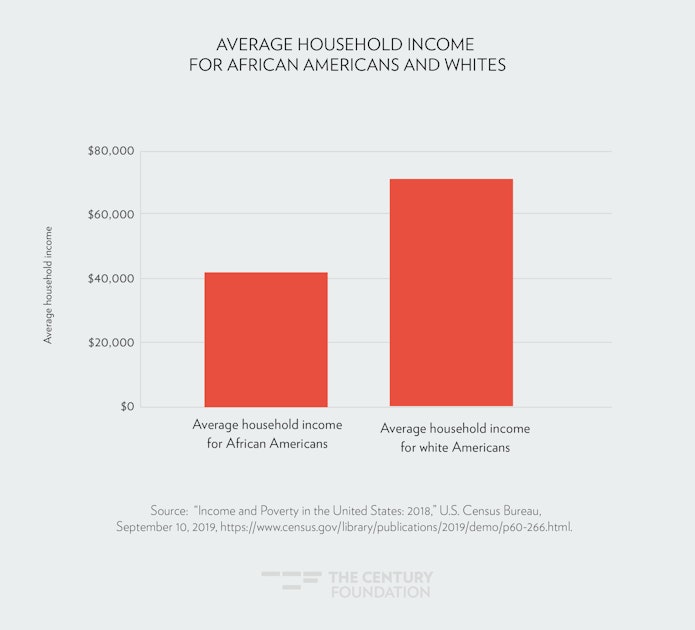
African-American households have significantly lower household income than white households. The average household income for African Americans in 2018 was $41,361, while it was $70,642 for white households.50 (See Figure 4.) African Americans tend to make less than whites for the same jobs, pointing to unequal pay as a contributing factor in the gap in household income.51 Even when taking into account similar education levels, workers of color are consistently paid less than white workers.52
Income is a major factor in a family’s ability to access health care, which can make up a significant share of household spending in terms of insurance premium costs and out-of-pocket costs.
Figure 4
The Wealth Gap
When it comes to accumulating wealth, the numbers are even more grim—white families now have approximately ten times the wealth of African-American families, on average.53 (See Figure 5.) Research shows that the wealth gap impacts African Americans across the income and education spectrum, making it harder for them to own homes or build retirement savings.54 And while African Americans on average have less total debt than whites, the wealth gap means they are more likely to have costly, high-interest debt obligations. High health care costs and surprise medical bills can negatively affect an African-American family’s ability to reduce or eliminate debt, and ultimately the ability to create wealth—which could impact a family for generations.
Figure 5

Food Insecurity
Food insecurity is also an issue affecting many African Americans and has important implications for health outcomes and economic well-being. Food insecurity occurs when a household or family lacks access to adequate nutritious food.55 This happens due to the lack of financial means to purchase healthy food or by living in impoverished geographic areas void of grocery stores with whole, fresh foods. Neighborhoods that lack access to nutritious foods are also referred to as food deserts.56 The ten U.S. counties with the highest food insecurity rates are all at least 60 percent African-American.57 African Americans experience hunger at twice the rate of white Americans, including one in four African-American children.58 Hunger can also lead to chronic illness and has been associated with low-birth weight, diabetes, cancer, pregnancy complications, and mental distress.59
The Lack of Safe and Affordable Housing
Housing and neighborhood safety are also important economic indicators that can impact health. Unfortunately, far too many African Americans have to grapple with neighborhood violence and environmental factors (such as a lack of clean water, exposure to lead paint, and pollution) that can negatively impact both their mental and physical health. Additionally, a relative lack of affordable housing options and home ownership continues to plague the African-American community, largely due to longstanding racist practices such as redlining and subprime mortgages. The lack of affordable housing puts a financial strain on families and can pull resources away from necessities like food and medical care.60 For homeless and transient communities, it can be almost impossible to access health care or maintain adequate health regimens. Despite comprising just 13.4 percent of the total U.S. population, African Americans make up 40 percent of the homeless population, and are an overrepresented part of this group in every state.61
Overview of Health Care Reform Plans
Several health care reform proposals62 have been introduced by members of U.S. Congress and by 2020 presidential candidates. In this section, the most widely known and promising plans that have gained traction and media coverage in recent months are highlighted.63
Medicare for All
Medicare for All is a signature single-payer plan originally authored by Senator Bernie Sanders, setting forth a vision for major structural change of the health insurance system. It has since been endorsed and supported by Representative Pramila Jayapal (who introduced the House version of the legislation), Representative Alexandria Ocasio-Cortez, Senator Elizabeth Warren, Senator Kamala Harris, Senator Cory Booker, and a host of other progressive policymakers.64 It calls for a single federal program with comprehensive benefits for all U.S. residents that would replace all private insurance, Medicaid, Medicare, and the Children’s Health Insurance Program (CHIP). The plan would be financed by taxes and eliminate premiums and cost-sharing or out-of-pocket costs, leading to major cost-savings for consumers in the long run. Taking into account the vast economic challenges for African Americans, savings in health care costs could help lead to better economic outcomes. In turn, health outcomes could also improve due to more comprehensive coverage available to all.
Comprehensive health benefits under Medicare for All include medically necessary services in thirteen benefit categories, including home and community-based long-term care, dental care, hearing, vision care, comprehensive reproductive health care (including abortion services), and transportation to health care appointments for people with disabilities and low-income people.65 Drug prices would be negotiated annually and a formulary would be established. Medicare for All would also prohibit balance billing, also known as surprise billing, which happens when health providers bill patients for the difference in the total cost of a health care service and the amount paid by an insurer.66
Public Insurance Option
Public option plans call for a federal insurance option. These plans essentially build upon the ACA by adding a new option available to those seeking coverage. Former vice president Joe Biden has been an advocate for this plan and has included it in his platform as a 2020 presidential candidate. There are several versions of the public option—some that would leave the marketplace subsidy structure unchanged, and others that would enhance it for all plan participants. Some public option proposals even go so far as to eliminate individual heath insurance plans created by the ACA. A key difference in the Biden plan, when compared with Medicare for All, is that it retains current public and private insurance sources. For people who like or prefer their private insurance, they can maintain it under the Biden plan.
The Biden plan would retain major components of the ACA including protections for people with pre-existing conditions, premium subsidies, and Medicaid expansion, along with offering public insurance as an option to anyone who wants it.67 A public insurance option was initially part of the ACA as introduced in Congress but was taken out of the legislation later in the negotiations process. Biden’s public option plan also aims to reduce the cost of prescription drugs by allowing importation of them from other countries, empowering Medicare to negotiate drug prices, and supporting the development of generic drugs.68 It would also offer tax credits to middle class families to help lower the cost of health insurance and eliminate the 400 percent federal poverty level income cap. The plan would eliminate balanced billing and be financed through capital gains taxes on rich individuals. Biden’s plan also includes protecting access to contraception and abortion rights, as well as the promise to adopt California’s strategy of public–private partnerships nationwide in addressing the U.S. maternal mortality crisis as major steps in building upon the ACA. Various versions of public insurance option legislation have also been introduced in Congress by Senator Ben Cardin, Representative Cedric Richmond, Senator Tim Kaine, Representative Jan Schakowsky, and others.
Sixty-one percent of white respondents in a November 2019 Gallup poll prefer the private health insurance system, whereas 57 percent of nonwhite respondents prefer government-run insurance.69 The cost of health care is still of major concern for those people with private health insurance, more so than for those with public insurance sources.70
Ensuring Health Care Access and Affordable Coverage for African Americans
The single payer and public option insurance plans outlined in this report were developed in a way to help fill coverage gaps and get as many people insured as possible. The plans aim to do this by emphasizing affordability—addressing the high cost of insurance premiums and limiting out-of-pocket costs, including surprise medical bills, prescription drugs, and fees for direct health care services. Unfortunately, current health reform plans fall short in adequately addressing racism in the health care system. This stands in the way of ensuring health equity, namely full insurance coverage and quality health care access for African Americans.
Cost to the individual is certainly an important factor in the conversation about health coverage and ensuring that people can access the health care services they need. However, in order for African Americans to attain meaningful insurance coverage and access to quality health care, the health care system must be transformed to better address the unique social factors that cause African Americans to remain in the coverage gap and how racism plays a role in their health outcomes. Furthermore, the economic challenges African Americans face serve as barriers to sustaining comprehensive coverage which can lead to poor health outcomes. It is simply not enough for insurance coverage to be affordable or even “free”—it must also serve as a tool in progress toward systemic change and equity that will help African Americans get ahead.
To do this, getting to universal health care coverage will require that the following steps be taken:
- Promote health equity by adequately addressing racism, bias, discrimination, and other systemic barriers within the health care system. To do this, policymakers must acknowledge the historical foundations of racism and ensure that health care providers, personnel and staff are substantively trained to recognize and eliminate all forms of bias in the health care system. Accountability measures at both the individual and systems levels should be in place, including measures that link payment, professional certification, and licensure to quality of care.
- Incorporate evidence-based tools to adequately address health disparities that focus on quality of care that extend beyond health insurance coverage, including the impact of racism on the health of African Americans throughout the life course. In health reform efforts, policymakers must take into account the social determinants and address how they impact health by working across sectors, including social support agencies and community-based providers with patient-centered approaches to care. Racist practices, such as those in the treatment and pain management of African Americans, should be eliminated.
- Protect and expanding access to insurance coverage and comprehensive benefits and bolstering the ACA benefit provisions and nondiscrimination guarantees. These efforts should include preserving coverage for people with pre-existing conditions by further codifying protections that ensure benefit inclusion and design decisions that do not result in limiting access to care. Policymakers should also build on the essential health benefits package to include important health care services currently omitted, such as long-term care and dental care.
- Protect the integrity of Medicaid, an important health insurance source for African Americans, by denying state efforts to impose draconian stipulations on coverage for enrollees such as work requirements. In order to close the coverage gap among African Americans, policymakers must also implement targeted strategies to incentivize and ensure Medicaid expansion in all southern states.
- Ensure access to quality providers and addressing provider shortages and hospital closures by anticipating increases in demand and working with HRSA to implement concrete strategies to close gaps in health care access for medically underserved areas/populations and health professional shortage areas. Strategies should include plans to not only increase the health care workforce, but also diversify it and offer technical support and training to minority-serving hospitals.
- Support the development of a robust, diverse, and culturally competent health care workforce by encouraging and facilitating diversity throughout the health care system and care teams, and adequately training all staff to be culturally sensitive. Payment rates and coverage guidelines for health care coverage should be developed in a way that supports fair, living wages and pay equity in the health care professions and jobs.
- Limit the cost of premiums and out-of-pocket costs, helping to make health insurance more affordable for individuals and families across the income spectrum. This should include limiting deductibles, prescription drug costs and other point-of-service charges, and completely eliminating surprise medical bills. All of these costs are major barriers to health care access, particularly for individuals and families with limited incomes.
- Strengthen access to trusted community-based providers currently available through safety-net programs, such as Medicaid, Medicare, and the Children’s Health Insurance Program (CHIP). These programs are often lifelines for marginalized communities and they disproportionately serve people of color. Policymakers should develop health reform plans that are intentional in ensuring continued access to these vital sources of care, as well as seamless coordination with health insurance payers for people with coverage seeking care from community-based providers.71
African Americans stand to make significant gains if health reform is done right. The statistics outlined in this report paint a grim picture. Regardless of the progress made in recent decades, far too many African Americans still struggle to lead healthy and economically secure lives. This is due to the long-standing effects of racism, which touches all African Americans, regardless of socioeconomic status. These effects can be reversed, but it will take real commitment and systemic change. Health care reform must be part of the effort.
Notes
- “Quick Facts, “ U.S. Census Bureau, accessed November 15, 2019, https://www.census.gov/quickfacts/fact/table/US#.
- Janel Jones, John Schmitt, and Valerie Wilson, “50 Years After The Kerner Commission, African Americans Are Better Off In Many Ways, But Are Still Disadvantaged By Racial Inequality,” Economic Policy Institute, February 26, 2018, https://www.epi.org/publication/50-years-after-the-kerner-commission/.
- Ibid.
- Bowen Garret and Anju Gangopadhyaya, “Who Gained Health Insurance Coverage Under the ACA, and Where Do They Live?” Urban Institute and Robert Wood Johnson Foundation, December 2016, https://www.urban.org/sites/default/files/publication/86761/2001041-who-gained-health-insurance-coverage-under-the-aca-and-where-do-they-live.pdf.
- “Health Insurance Coverage in the United States: 2018,” U.S. Census Bureau, November 2019, https://www.census.gov/content/dam/Census/library/publications/2019/demo/p60-267.pdf.
- Ibid.
- “The Real Cost of Health Care: Interactive Calculator Estimates Both Direct and Hidden Household Spending,” Henry J. Kaiser Family Foundation, February 21, 2019, https://www.kff.org/health-costs/press-release/interactive-calculator-estimates-both-direct-and-hidden-household-spending/.
- Calculated by the author using the average annual household income for African Americans ($41,361) and the annual health care premium cost for families ($8,200).
- U.S. Census Bureau, “Health Insurance Coverage In The United States.”
- “Key Facts About the Uninsured Population,” Henry J. Kaiser Family Foundation, December 7, 2018, https://www.kff.org/uninsured/fact-sheet/key-facts-about-the-uninsured-population/.
- Sara R. Collins, Herman K. Bhupal, and Michelle M. Doty, “Health Insurance Coverage Eight Years After The ACA: Fewer Uninsured Americans and Shorter Coverage Gaps,” The Commonwealth Fund, February 7, 2019, https://www.commonwealthfund.org/publications/issue-briefs/2019/feb/health-insurance-coverage-eight-years-after-aca.
- “Program History: Medicaid,” Centers for Medicare and Medicaid Services, accessed November 16, 2019, https://www.medicaid.gov/about-us/program-history/index.html.
- “Medicaid and Medicare Are Important to African Americans,” National Committee to Preserve Social Security and Medicare, January 28, 2019, https://www.ncpssm.org/documents/medicare-policy-papers/medicare-medicaid-important-african-americans/.
- Rachel Garfield, Kendal Orgera, and Anthony Damico, “The Coverage Gap: Uninsured Poor Adults in States that Do Not Expand Medicaid,” Henry J. Kaiser Family Foundation, March 21, 2019, https://www.kff.org/medicaid/issue-brief/the-coverage-gap-uninsured-poor-adults-in-states-that-do-not-expand-medicaid/.
- “Overview of the Affordable Care Act and Medicaid,” Medicaid and CHIP Payment and Access Commission, accessed November 17, 2019, https://www.macpac.gov/subtopic/overview-of-the-affordable-care-act-and-medicaid/.
- National Federation of Independent Business v. Sebelius, 567 U.S. 519 (2012).
- Section 1115 Medicaid demonstration waivers allow states to test new approaches in Medicaid that differ from what is required by federal statute. “Medicaid Expansion to the New Adult Group,” Medicaid and CHIP Payment and Access Commission, accessed November 17, 2019, https://www.macpac.gov/subtopic/medicaid-expansion/.
- “Profile: African Americans.”
- Peggy Bailey, Matt Broaduss, Shelby Gonzales, and Kyle Hayes, “African American Uninsured Rate Dropped by More Than a Third Under the Affordable Care Act: Repealing ACA and Cutting Medicaid Would Undercut Progress,” Center on Budget and Policy Priorities, June 1, 2017, https://www.cbpp.org/research/health/african-american-uninsured-rate-dropped-by-more-than-a-third-under-affordable-care.
- “State Proposals for Medicaid Work and Community Engagement Requirements,” National Academy for State Health Policy, accessed November 19, 2019, https://nashp.org/wp-content/uploads/2018/01/Medicaid-Work-Requirements-Chart_10_31_19_Final.pdf.
- Phil Galewitz, “Study: Arkansas Medicaid Work Requirement Hits Those Already Employed,” Kaiser Health News, June 19, 2019, https://khn.org/news/study-arkansas-medicaid-work-requirements-hit-those-already-employed/.
- Judith Solomon, “Medicaid Work Requirements Can’t Be Fixed: Unintended Consequences Are Inevitable Result,” Center on Budget and Policy Priorities, January 10, 2019, https://www.cbpp.org/research/health/medicaid-work-requirements-cant-be-fixed.
- “America’s Health Rankings: 2018 Annual Report,” United Health Foundation, https://www.americashealthrankings.org/learn/reports/2018-annual-report/findings-state-rankings; “Rural Health Disparities,” Rural Health Information Hub, accessed November 17, 2019, https://www.ruralhealthinfo.org/topics/rural-health-disparities.
- Laurie McGinley, “ACA Linked to Reduce Racial Disparities, Earlier Diagnosis and Treatment in Cancer Care: New Research Backs Up Earlier Data Showing the Law Increased Access to Care,” Washington Post, June 2, 2019, https://www.washingtonpost.com/health/2019/06/02/aca-linked-reduced-racial-disparities-earlier-diagnosis-treatment-cancer-care/.
- Emily E. Peterson, Nicole L. Davis, David Goodman, Shannon Cox, and others, “Racial/Ethnic Disparities in Pregnancy-Related Deaths—United States 2007–2016,” Centers for Disease Control and Prevention, September 6, 2019, https://www.cdc.gov/mmwr/volumes/68/wr/mm6835a3.htm?s_cid=mm6835a3_w.
- “Infant Health Mortality and African Americans,” U.S. Department of Health and Human Services Office of Minority Health, accessed November 17, 2019, https://minorityhealth.hhs.gov/omh/browse.aspx?lvl=4&lvlid=23.
- “African American Death Rate Drops 25 Percent,” Centers for Disease Control and Prevention, May 2, 2017, https://www.cdc.gov/media/releases/2017/p0502-aa-health.html.
- Ibid.
- Yolanda T. Mitchell and Tiffany L. Bromfield, “Gun Violence and the Minority Experience,” National Council on Family Relations, January 10, 2019, https://www.ncfr.org/ncfr-report/winter-2018/gun-violence-and-minority-experience.
- Darrell J. Gaskin, Gniesha Y. Dinwiddie, Kitty S. Chan, and Rachel McCleary, “Residential Segregation and Disparities in Healthcare Services Utilization,” Medical Care Research and Review, April 2012, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3387667/; Darrell J Gaskin, Gniesha Y. Dinwiddie, Kitty S. Chan, and Rachael R McCleary, “Residential Segregation and the Availability of Primary Care Physicians,” Health Services Research 47, no. 6 (December 2012): 2353–76, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3416972/.
- Ibid.
- “Health Professional Shortage Areas,” Health Resources and Services Administration, accessed November 19, 2019, https://bhw.hrsa.gov/shortage-designation/hpsas.
- “Primary Care Health Professional Shortage Areas,” Henry J. Kaiser Family Foundation, accessed November 19, 2019, https://www.kff.org/other/state-indicator/primary-care-health-professional-shortage-areas-hpsas/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D.
- “Explore Data and Maps on HRSA’s Health Care Programs,” Health Resources and Services Administration, accessed November 19, 2019, https://data.hrsa.gov/.
- “Medically Underserved Areas and Populations,” Health Resources and Services Administration, accessed November 19, 2019, https://bhw.hrsa.gov/shortage-designation/muap.
- Ibid.
- University of Southern California, “Racism has a toxic effect: Study may explain how racial discrimination raises the risks of diseas among African Americans,” Science Daily, May 31, 2019, https://www.sciencedaily.com/releases/2019/05/190531100558.htm.
- April D. Thames, MIchael R. Irwin, Elizabeth C. Breen, and S.W. Cole, “Experienced Discrimination and Racial Differences in Leukocyte Gene Expression,” Psychonueroendocrinology, August 2019, https://www.sciencedirect.com/science/article/abs/pii/S0306453018310436?via%3Dihub.
- Ibid.
- University of Southern California, “Racism has a toxic effect.”
- Arline T. Geronimus, Margaret Hicken, Danya Keene, and John Bound, “Weathering” and Age Patterns of Allostatic Load Scores Among Blacks and Whites in the United States,” American Journal of Public Health, May 2006, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1470581/.
- Bruce S. McEwen, “Protective and Damaging Effects of Stress Mediators,” Seminars in Medicine of the Beth Israel Deaconess Medical Center, New England Journal of Medicine, January 15, 1998.
- Ziad Obermeyer, Brian Powers, Christine Vogeli, and Sendhil Mullainathan, “Dissecting Racial Bias in an Algorithm Used to Manage the Health of Populations,” Science, October 25, 2019, https://science.sciencemag.org/content/366/6464/447; Kelly M. Hoffman, Sophie Trawalter, Jordan R. Axt, M. Norman Oliver, “Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between blacks and whites,” Proceedings of the National Academy of Sciences of the United States of America, April 4, 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4843483/.
- See, for example, Kelly M. Hoffman, Sophie Trawalter, Jordan R. Axt, and M. Norman Oliverb, “Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between blacks and whites,” Proceedings of the National Academy of Science 113, no. 16 (April 19, 2016): 4,296–301, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4843483/; Darcell P. Scharff, Katherine J. Mathews, Pamela Jackson, Jonathan Hoffsuemmer, Emeobong Martin, and Dorothy Edwards, “More than Tuskegee: Understanding Mistrust about Research Participation,” Journal of Health Care for the Poor and Underserved 21, no. 3 (August 2010): 879–97, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4354806/; and Ziad Obermeyer, Brian Powers, Christine Vogeli, and Sendhil Mullainathan, “Dissecting racial bias in an algorithm used to manage the health of populations,” Science 366, no. 6,464 October 25, 2019): 447–53, https://science.sciencemag.org/content/366/6464/447
- Dwyane T. Brandon, Lydia A. Isaac, and Thomas A. LaVeist, “The legacy of Tuskegee and trust in medical care: is Tuskegee responsible for race differences in mistrust of medical care,” Journal of the National Medical Association, July 2005, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2569322/.
- “Economic News Release: Employment status of the civilian population by race, sex, and age,” U.S. Department of Labor Bureau of Labor Statistics, accessed November 18, 2019, https://www.bls.gov/news.release/empsit.t02.htm; Janelle Jones, “In 14 states and DC, the African American unemployment rate is at least twice the white unemployment rate,” Economic Policy Institute, May 17, 2018, https://www.epi.org/publication/state-race-unemployment-2018q1/.
- U.S. Census Bureau, Current Population Survey, 2018 and 2019 Annual Social and Economic Supplements (CPS ASEC).
- “The Impact of Poverty, Food Insecurity, and Poor Nutrition on Health and Wellbeing,” Food Research and Action Center, December 2017, https://frac.org/wp-content/uploads/hunger-health-impact-poverty-food-insecurity-health-well-being.pdf.
- “Medicaid Expansion Helps Address Health Disparities,” Centers for Medicare and Medicaid Services, accessed November 18, 2019, https://www.medicaid.gov/about-us/program-history/medicaid-50th-anniversary/?entry=47671.
- “Income and Poverty in the United States: 2018,” U.S. Census Bureau, September 10, 2019, https://www.census.gov/library/publications/2019/demo/p60-266.html.
- Brentin Mock, “How Income Inequality Feeds the Racial Wealth Gap,” Citylab, March 21, 2019, https://www.citylab.com/equity/2019/03/racial-wealth-gap-income-inequality-black-white-households/585325/.
- Ibid.
- Angela Hanks, Danyelle Solomon, and Christian E. Weller, “Systemic Inequality: How America’s Structural Racism Helped Create the Black-White Wealth Gap,” Center for American Progress, February 21, 2018, https://www.americanprogress.org/issues/race/reports/2018/02/21/447051/systematic-inequality/.
- Ibid.
- Craig Gundersen and James P. Ziliak, “Food Insecurity And Health Outcomes,” Health Affairs, November 2015, https://www.healthaffairs.org/doi/full/10.1377/hlthaff.2015.0645.
- “USDA Defines Food Deserts,” American Nutrition Association, accessed October 1, 2019, http://americannutritionassociation.org/newsletter/usda-defines-food-deserts.
- “African American Hunger and Poverty Facts,” Feeding America, accessed October 1, 2019, https://www.feedingamerica.org/hunger-in-america/african-american.
- Ibid.
- “The Impact of Poverty.”
- P. Braveman, M. Dekker, S. Egerter, T. Sadegh-Nobari, and C. Pollack, “How Does Housing Affect Health: An Examination of the Many Ways Housing Can Influence Health and Strategies To Improve Health Through Emphasis on Healthier Homes,” Robert Wood Johnson Foundation, May 1, 2011, https://www.rwjf.org/en/library/research/2011/05/housing-and-health.html.
- Joy Moses, “Demographic Data Project: Race, Ethnicity, and Homelessness,” National Alliance to End Homelessness—Homelessness Research Institute, accessed November 17, 2019, https://endhomelessness.org/wp-content/uploads/2019/07/3rd-Demo-Brief-Race.pdf.
- Jeanne Lambrew and Jennifer MIshory, “Comparison of Health Reform Legislation Creating Public Plans,” The Century Foundation, August 7, 2019, https://tcf.org/content/commentary/comparison-health-reform-legislation-creating-public-plans/.
- Luna Lopes, Liz Hamel, Audrey Kearny, and Mollyann Brodie, “KFF Health Tracking Poll—October 2019: Health Care in the Democratic Debates, Congress, and the Courts,” Henry J. Kaiser Family Foundation, October 15, 2019, https://www.kff.org/health-reform/poll-finding/kff-health-tracking-poll-october-2019/.
- H.R. 1384, Medicare for All, accessed November 18, 2019, https://www.congress.gov/116/bills/hr1384/BILLS-116hr1384ih.pdf.
- Ibid.
- “Balanced Billing,” U.S. Centers for Medicare and Medicaid Services—HealthCare.gov, accessed November 17, 2019, https://www.healthcare.gov/glossary/balance-billing/.
- Dan Diamond, “Biden Unveils Health Care Plan: Affordable Care Act 2.0,” Politico, July 15, 2019, https://www.politico.com/story/2019/07/15/joe-biden-health-care-plan-1415850.
- Ibid., and “Health Care,” Joe Biden For President, accessed November 18, 2019, https://joebiden.com/healthcare/.
- Gallup News poll conducted November 1–14, 2019, available for download from https://news.gallup.com/file/poll/268988/191204GovtResponsibility.pdf.
- Tami Luhby, “Americans are still pretty happy with their private health insurance,” CNN, December 9, 2019, https://www.cnn.com/2019/12/09/politics/gallup-private-health-insurance-satisfaction/index.html.
- For additional recommendations, please see Jamila Taylor and Jen Mishory, “Health Reform’s North Star: 10 Guidelines to Reach Universal Health Care Coverage,” The Century Foundation, November 13, 2019, https://tcf.org/content/commentary/health-reforms-north-star-10-guidelines-reach-universal-health-care-coverage/.









